The Hidden Foundation
Visible Medicine Rests on an Invisible Foundation
When we think about medicine, we see the interventions — surgery, diagnostic imaging, pharmaceuticals, intensive care. These are what patients and families recognize as "treatment." But beneath every successful NICU outcome lies an invisible infrastructure that rarely earns the same recognition: standardized protocols, nursing consistency, team communication, quality improvement processes, evidence-based guidelines, and a culture of safety.
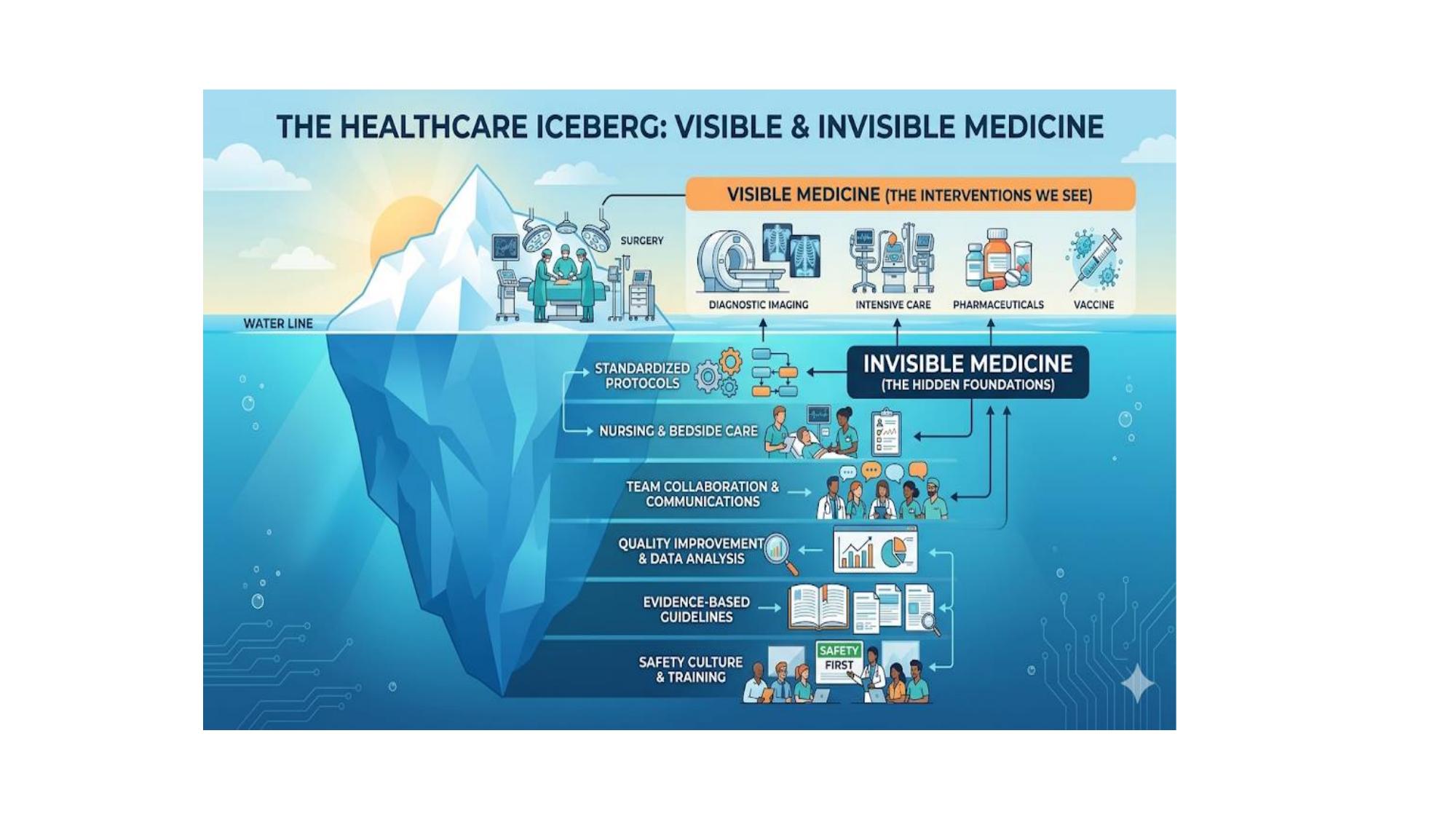
The Healthcare Iceberg: visible interventions — surgery, imaging, pharmaceuticals — rest on a vast invisible foundation of standardized protocols, nursing care, quality improvement, evidence-based guidelines, and safety culture. In neonatology, this invisible layer is where outcomes are shaped.
"In neonatology, consistency of care is often described as the 'invisible medicine.' Because the evidence base is thin, the variation in practice — the difference in how two different doctors might treat the same baby — becomes a significant concern in itself."
— NeoGuide Collective, Consistency of Care FrameworkWhen care is inconsistent, we are introducing uncontrolled variability into the care of the most fragile patients in medicine. And unlike in adult care, where patients can often compensate for physiologic disruption, neonates — especially those born extremely preterm — cannot.
The Research Landscape
Why Neonatology Faces a Uniquely Difficult Evidence Problem
Every specialty grapples with uncertainty, but neonatology faces structural barriers to evidence generation that set it apart from virtually every other field in medicine. Understanding these barriers is essential to understanding why consensus-based approaches are not a fallback — but represent another parallel path forward.
The barriers to evidence generation in neonatology are formidable and well-documented. Enrolling vulnerable newborn populations in RCTs carries significant ethical and liabilities, with complex parental consent requirements. Physiological complexity means that a drug safe at 32 weeks gestation may be toxic at 24 weeks. Small market size reduces pharmaceutical incentive to fund large-scale trials. And the true measure of success in neonatology — neurodevelopmental outcome at age 2, 5, or even 18 — makes longitudinal studies expensive and difficult to sustain.
The result is stark: pulmonary surfactant remains essentially the only drug ever developed specifically for neonates. For everything else — the ventilator strategies, the transfusion thresholds, the nutrition protocols, the medication dosing — we are operating largely on expert judgment, institutional tradition, and extrapolation from older children and adults.
The Four Barriers to Evidence in Neonatology
Why neonatology has so few definitive trials
-
Ethical Constraints Enrolling vulnerable newborn populations in RCTs carries significant ethical and liability concerns, with complex parental consent requirements.
-
Physiological Complexity Rapidly developing organ systems mean evidence from 32-weekers may not apply to 24-weekers.
-
Small Market Size Many neonatal conditions qualify as “rare diseases,” reducing pharmaceutical companies’ financial incentive to fund large-scale trials.
-
Long-term Follow-up The true measure of neonatal outcomes — neurodevelopmental health at age 2, 5, or 18 — makes longitudinal research extraordinarily expensive.
This is not a failure of individual clinicians or institutions. It is a structural problem — and it demands a structural solution. That solution begins with standardization: creating the common clinical language, shared protocols, and collaborative infrastructure that can turn the daily care of thousands of neonates across hundreds of NICUs into a living, continuously updated evidence base.
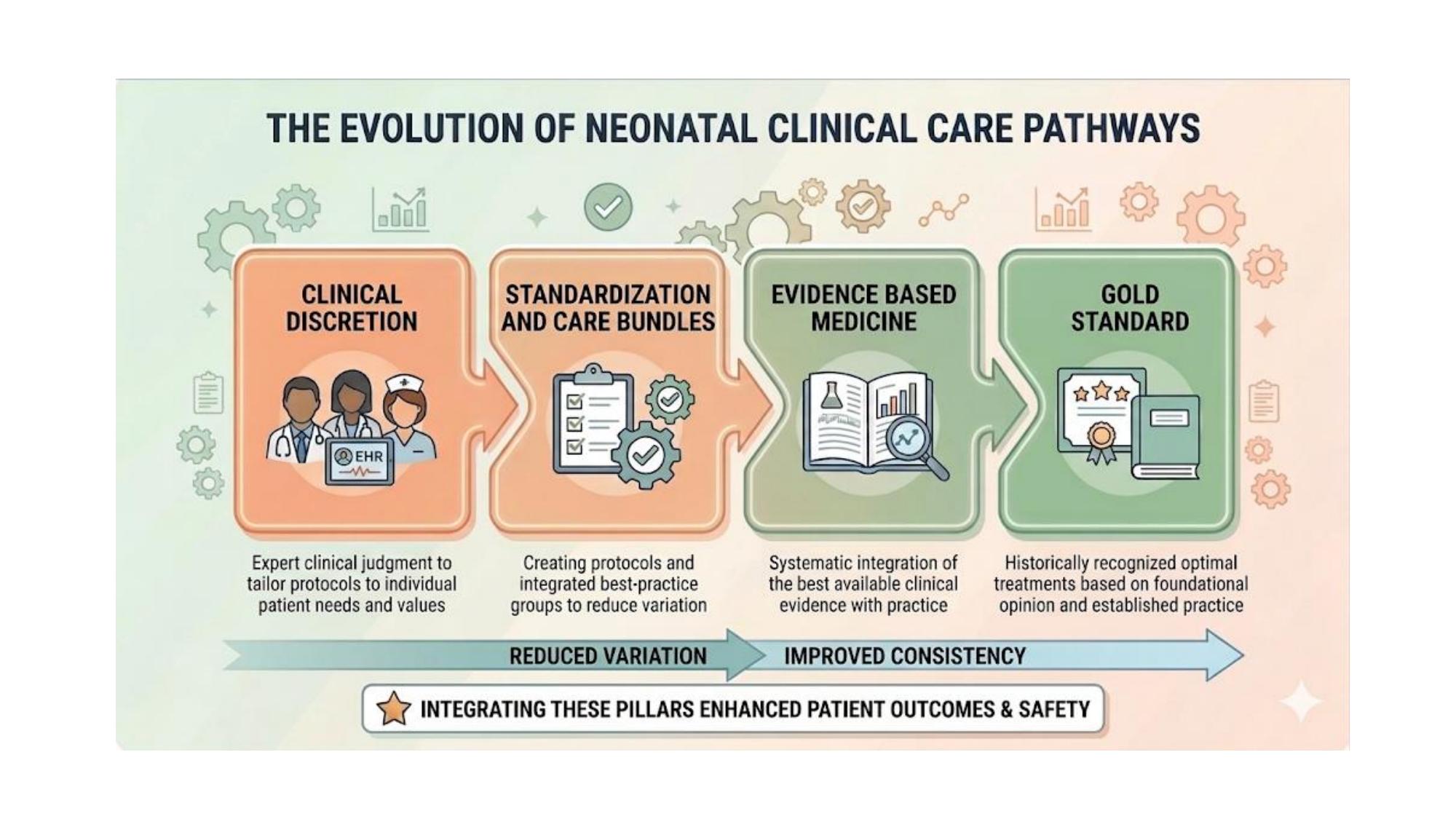
The evolution of neonatal clinical care pathways: from individual clinical discretion toward standardization and care bundles, evidence-based medicine, and ultimately gold-standard integrated practice. Integrating these pillars enhances patient outcomes and safety — with reduced variation and improved consistency as the bridge between them.
The Science of Consistency
What Inconsistency Actually Does to a Neonate
The argument for consistency of care is not merely philosophical. There is a growing body of evidence demonstrating that variation in neonatal practice causes measurable, physiologically strain — even when each individual clinical decision, viewed in isolation, appears reasonable.
Physiologic Stability and the Developing Brain
Preterm infants have extremely fragile autoregulatory systems. Their ability to maintain stable cerebral blood flow, blood pressure, temperature, and oxygenation is tenuous at best. When care varies — when ventilator settings are adjusted differently by the morning and evening physician, when fluid management protocols shift between providers, when handling styles change with staff turnover — the resulting physiologic fluctuations are not trivial.
Emerging research shows that consistency extends beyond physiology into neurodevelopment. Infants with predictable caregivers demonstrate better cognitive and social-emotional development. A baby's brain begins forming "expectations" based on caregiver response patterns remarkably early. Even babies recognize consistency in their care.
The Noise Reduction Effect
Consistency also has a critical diagnostic benefit that is often overlooked. In a NICU where everyone follows a different clinical "hunch," it becomes nearly impossible to distinguish a baby's underlying illness trajectory from the noise created by inconsistent management. When care is standardized, a baby's deviation from the established baseline — a feeding intolerance, a subtle change in respiratory pattern, an unexpected vital sign trend — becomes immediately recognizable as a signal. Consistency creates the quiet background against which early complications like sepsis or NEC can be detected far sooner.
"Consistency creates a stable 'baseline' that allows teams to spot complications like sepsis or NEC much faster, because the baby's deviation from the norm is more obvious."
— NeoGuide Consistency of Care FrameworkThe Problem of Uncertainty — and What It Does to Clinicians
Uncertainty in neonatology is not just a patient safety issue — it is a workforce wellness issue. A 2025 national survey of neonatologists revealed that uncertainty is a primary driver of clinician stress, moral distress, and communication difficulties. Early-career neonatologists report the highest levels of discomfort with ambiguity. Many feel what researchers describe as a "Hippocratic push" — the fear that if they standardize care and a bad outcome occurs, they may have "given up" on a baby who could have done better with a different approach.
This is the paradox at the heart of neonatal uncertainty: the very fear of standardization — rooted in genuine care for individual patients — can perpetuate the variation that makes individual patients worse off. Consensus building is the mechanism that resolves this paradox. When clinicians collectively agree on an approach, each individual is relieved of the burden of solo uncertainty. The decision becomes shared, the evidence becomes collective, and the moral weight is distributed across the community.
| Feature | Evidence-Based Practice (EBM) | Consistency-Based Practice (Standardization) |
|---|---|---|
| Driver | Large-scale RCTs / Meta-analyses | Local Protocols / Care Bundles |
| Goal | Finding the "Best" Treatment | Eliminating Harmful Variation |
| Benefit | Clinical Efficacy | Physiological & Neurological Stability |
| Philosophy | "Follow the science." | "Reduce the noise." |
These two approaches are not in competition — they are complementary pillars of excellent neonatal care. Where high-certainty evidence exists, we follow it. Where it does not — which in neonatology means the vast majority of clinical decisions — standardization based on the best available expert consensus is not a compromise. It is the most scientifically defensible approach available.
Proven in Practice
Consensus-Driven Standardization Has Already Changed Medicine
Skeptics of standardization sometimes argue that consensus-based guidelines "turn doctors into robots" — that they subordinate clinical judgment to bureaucratic protocol. The evidence from across medicine tells a very different story. In field after field, consensus-driven standardization has not eliminated excellent clinical care; it has rescued it from the chaos of uncoordinated variation.
ARDS and Prone Positioning
For decades, acute respiratory distress syndrome (ARDS) carried a mortality rate of 40–50%. The evidence for individual interventions was mixed and contested. When the European Society of Intensive Care Medicine and the American Thoracic Society issued a consensus guideline for early prone positioning in severe cases — based largely on expert consensus rather than definitive RCT evidence — hospitals that adopted the standardized "triggers" for flipping patients saw significant reductions in ventilator-induced lung injury and improved oxygenation. The consensus did not create new biology. It eliminated the variation that was preventing a known beneficial intervention from being applied consistently.
The Difficult Airway Algorithm
One of the most dangerous moments in clinical medicine is a patient who cannot be intubated or ventilated. Before the American Society of Anesthesiologists created the Difficult Airway Algorithm using Delphi-style consensus, clinicians often made repeated failed intubation attempts — causing progressive trauma, swelling, and eventual cardiac arrest. The consensus statement introduced a simple "Stop-Point": if you fail twice, you must move to the next device or a surgical airway. The algorithm virtually eliminated "death by persistence" — not by creating new technology, but by replacing individual ego-driven decision-making with a standardized if-then flowchart. Brain damage from airway mishaps dropped significantly.
In Neonatology: Feeding Protocols and NEC
The neonatal evidence for standardization is growing. Feeding is perhaps the domain with the strongest evidence: necrotizing enterocolitis (NEC) has a well-documented iatrogenic component related to practice variation. Aggressive or inconsistent feeding advancements, changing thresholds for feeding intolerance, and inconsistent use of fortification all contribute to NEC risk. Evidence-based standardized feeding protocols consistently result in decreased time to full feeds and, critically, reduced NEC incidence. The 2023 "SIMPLE" Initiative demonstrated that milestone-targeted feeding plans — applied consistently across a unit — minimized variability and allowed for highly predictable discharge dates based on feeding milestones.
Similarly, standardizing the transition to non-invasive ventilation (NIPPV) has been shown to reduce the risk of bronchopulmonary dysplasia (BPD) and mortality compared to high-variance management. Standardized developmental care — consistent minimal disruption, noise control, positioning — improves neurodevelopmental scores at 9–12 months and reduces hospital costs.
"A consistent algorithm is safer than a 'brilliant' individual clinician acting on a whim — even when the evidence is 'messy.'"
— The NeoGuide CollectiveThe NeoGuide Approach
Building Consensus Together: The Community Effect
The most important insight from recent neonatology literature is that the benefit of standardization is not just in the protocol itself — it is in what the protocol enables. When multiple NICUs follow the same standard, they can share data more effectively. Every patient encounter becomes a standardized data point. The "n-of-1" problem — rare complications that don't happen often enough in a single hospital to study — dissolves when dozens of NICUs are collecting data using the same definitions, the same triggers, the same outcome measures.
This is what researchers describe as a Virtual Community of Practice (VCoP): a social-technical structure where clinicians across different hospitals use standardized protocols as a "common language" to share data, troubleshoot in real time, and generate evidence together. The global network of NICUs becomes, in effect, a continuous, live clinical trial — one capable of generating the Real-World Evidence (RWE) needed to fill the gaps that traditional RCTs cannot reach.
The objection that standardization "turns doctors into robots" misunderstands what true clinical autonomy means. True clinical autonomy is the ability to make a meaningful choice when the answer is known. In neonatology, where the answer is so often unknown, "unregulated autonomy" is not freedom — it is uncoordinated variation dressed up as expertise. The VCoP model reclaims genuine professional autonomy by involving clinicians in the creation and refinement of the standards themselves, rather than simply following mandates handed down from above.
The Modified Delphi Method: Consensus in Practice
NeoGuide uses the Modified Delphi Method as the core mechanism for building consensus. This is a systematic, iterative approach in which expert stakeholders — physicians, nurses, respiratory therapists, pharmacists, social workers, nutritionists, and families — are brought together around a specific clinical question. Surveys using a 9-point Likert scale identify areas of agreement (score >7), near-consensus (>6.5), and active disagreement (<6.5). Repeated rounds, guided by aggregate feedback, progressively narrow the scope of disagreement until a workable consensus emerges.
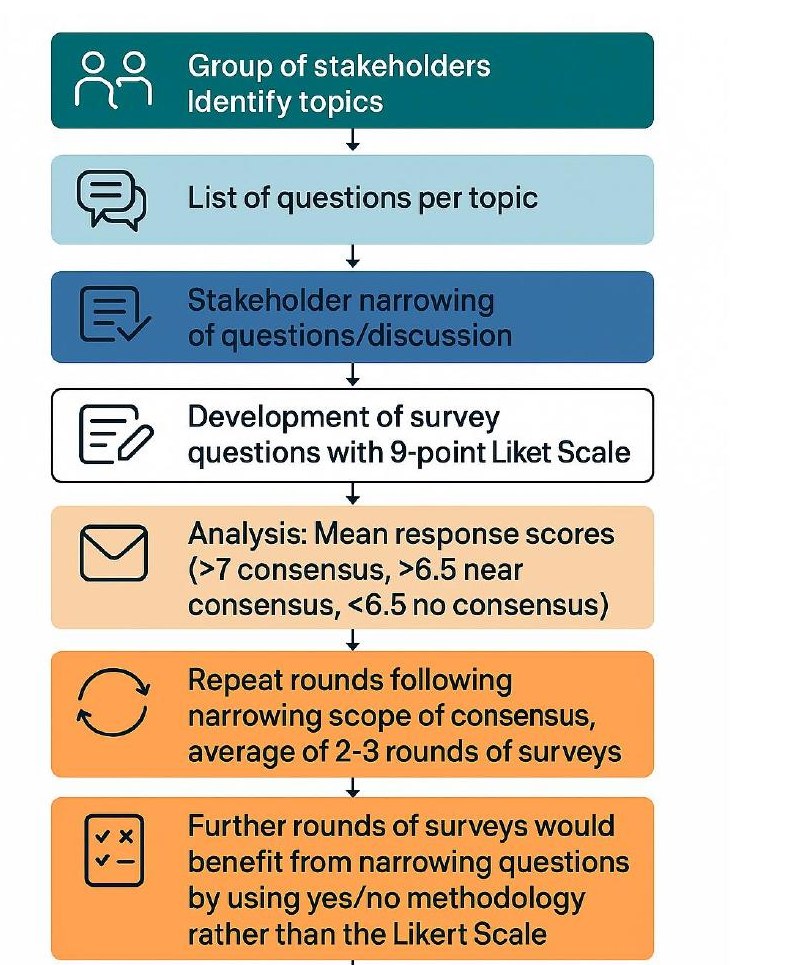
The Modified Delphi consensus process: stakeholders identify topics, narrow questions through structured discussion, and respond to surveys using a 9-point Likert scale. Analysis identifies consensus (mean >7), near-consensus (>6.5), and no consensus (<6.5). The process runs 2–3 rounds, with later rounds shifting to yes/no methodology to sharpen resolution.
The strength of the Modified Delphi process is that it does not require certainty — it requires structured dialogue. It converts the silent, uncoordinated variation of individual clinical judgment into an explicit, documented, community-owned position. When a unit implements a consensus-derived protocol, every clinician who contributed to that consensus becomes a stakeholder in its success, and every patient outcome becomes a data point for its refinement.

The NeoGuide Consensus Development Process: Team Formation (identify members, define scope, divide labor) → Evidence Gathering (literature search, identify expertise areas) → Small Group Work (goal-specific groups, narrowed literature search) → Optional Delphi Process → Finalization and Presentation (consensus recommendation, clinical presentation and broad validation).
What the Evidence Gap in Neonatology Actually Requires
Roles across the field
-
Hospital Leaders Invest in digital infrastructure that allows NICUs to share anonymized outcomes data in real time, creating the Common Clinical Language that makes multi-center learning possible.
-
Researchers In addition to RCTs, embrace multi-center Quality Improvement networks, where standardized practice generates the natural experiments.
-
Clinicians Recognize that the evidence gap is not a scientific failure but a structural one — and that participating in consensus building is itself a form of evidence generation.
-
Trainees Learn Systems Thinking and Collaborative Improvement as core competencies alongside clinical skills, understanding that individual excellence and collective standardization are partners, not opposites.
Join the Effort
NeoGuide is building the national framework for neonatal consensus and consistency of care. Whether you lead a Level II community NICU or a Level IV academic center, your practice patterns, your expertise, and your data matter.
Express Interest in NeoGuide